journal entry
May 09
2018
The Power of PARP Inhibition




"The cure for cancer" has long been a hot topic in science, politics and the media. It is one of those phrases, however, that as a scientist frustrates me because cancer is not just one disease. The recent pushes toward precision medicine and to understand the diverse landscape of cancers have reinforced this idea that every cancer is unique. Cancers used to be classified and treated based on the organ of origin (i.e., breast cancer, prostate cancer, ovarian cancer) and how they looked. Research into underlying genetic contributions to cancer, such as the roles of the BRCA1 and BRCA2 genes, however, is beginning to change how we classify and treat these diseases.
In addition to the organ in which they originate, cancers may be classified in many other ways, including by the tissue in which they develop — carcinoma, sarcoma, lymphoma, etc. Cancers may also be classified by the presence or absence of certain markers that distinguish them from normal cells around them. Breast cancers, for instance, can be positive or negative for the tumor markers HER2, ER and PR, which are proteins created by cells.
Each of these markers can be the target of a particular cancer treatment; it is any combination of these defining characteristics that dictates how a cancer is uniquely treated. New technology over the past decade, however, has also enabled us to analyze the DNA of cancer cells. Studying how the DNA of cancer cells differs from normal cells at a genetic level has provided a deeper understanding of the underlying causes of cancer. Consequently, we now classify cancers by genetic markers in addition to the physical ones. These analyses are teaching us that cancers with the same genetic mutations can arise in many different organs or tissues. Cancers that arise from mutated BRCA1 or BRCA2 genes, for instance, can develop in the breast, ovary, prostate, or pancreas, among other organs. BRCA-mutation status, therefore, comprises a different way to categorize a cancer: by genetic make-up rather than solely by physical characteristics.
Using Genetics to Target Cancer Treatment
Many cancer therapies can also affect the non-cancerous cells in the body. These treatments that also effect healthy cells often target markers that are characteristic, but not necessarily causative, of the cancer. The basis of why and how a cancer develops is determined by the difference in the genetic makeup of cancerous and non-cancerous cells. Understanding these differences, therefore, can allow doctors to treat the cancer cells specifically, with little-to-no effect on the healthy cells around them.
While BRCA-mutations can cause cancers across different tissues, organs and classifications of markers, the one thing they have in common is their defect in DNA repair. Scientists have figured out a way to exploit the genetic deficiency caused by BRCA mutations to treat only the cancer cells without harming the healthy ones. Drug treatments called PARP inhibitors do just that and are a targeted approach to treating cancers spanning many classifications (i.e., ovarian, breast) because of a common genetic deficiency in the BRCA genes. Categorizing cancers based on their genetic landscapes, therefore, will enable the development of treatments with broader applications than those that target the physical characteristics of a cancer.
Dr. Alan Ashworth[1], President of the UCSF Helen Diller Family Comprehensive Cancer Center and Co-leader of the UCSF Center for BRCA Research, with his laboratory of scientists was the first to discover a way to take advantage of the dysfunction of BRCA1- or BRCA2-mutated cells as a means of treating cancer. In 2005, Dr. Ashworth’s laboratory found that cells lacking the function of what is called a PARP protein were unable to normally repair DNA damage. These cells, instead, activated a backup repair pathway, involving BRCA1 and BRCA2, called HR (you can read my previous post, BRCA: Bracing the Genome, for a refresher on how BRCA1 and BRCA2 function in the HR pathway to seamlessly repair DNA breaks).
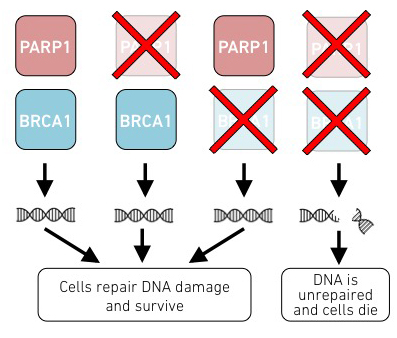
The researchers in Dr. Ashworth’s laboratory hypothesized that cells lacking PARP function AND either BRCA1 or BRCA2 function would compromise the ability of the cells to repair the damage, causing the cells to die. When the scientists found that cells lacking the function of both proteins died while cells lacking function of either PARP or one of the BRCA proteins survived, they began to inquire whether this could be a new way to treat cancers by targeting specifically the cancer cells without BRCA function.
What are PARPs?
Prior to Dr. Ashworth and his colleagues discovering that loss of PARP function in combination with loss of either BRCA1 or BRCA2 function was lethal to cells, PARP proteins were being targeted as a cancer treatment for non-BRCA-specific cancers. PARP proteins (in particular PARP1 and PARP2), like BRCA1 and BRCA2, help repair specific types of DNA damage in the cell. Unlike BRCA1 and BRCA2, however, PARPs aid in the repair of a different type of DNA damage: single-stranded breaks.
BRCA1 and BRCA2, on the other hand, are involved in the HR repair pathway that seamlessly repairs double-strand breaks — breaks in both strands of the DNA double helix (like breaking a ladder in half). HR repair is dependent on the newly replicated DNA and occurs during the latter part of the cell cycle[2]. PARP proteins are involved in the repair of single-strand breaks in the DNA double helix that occur prior to DNA replication. Similar to the functions of BRCA1 and BRCA2, PARP proteins are involved in signaling the proper repair proteins to do their job, not in the physical repair of the break. PARPs add tags to proteins that send out signals, like radars, to let other proteins know there is a problem in the cell. Because PARPs help repair breaks that occur before DNA replication, they function prior to the BRCA1/BRCA2-dependent HR repair pathway. If PARP proteins cannot fix DNA damage early in the cell cycle, the damage gets worse and needs to be fixed through a different mechanism.
Dr. Ashworth and his colleagues found that if this early repair pathway is not functional — for instance, if PARPs are inhibited with a drug — these single-stranded breaks persist. As DNA replication occurs, the machinery that builds the new DNA strand runs into the break. The collision exacerbates the damage, creating a double-strand break. Once the cell senses this new type of damage, it tries to repair it through the HR repair pathway. The need to fix a new type of DNA damage because the original damage is worsened is comparable to the brakes failing in your car, causing you to crash. After the crash, the brake failure becomes a moot point — you have to either fix the whole car or get rid of it and get a new one.
Once double-strand breaks are detected, a repair-or-die decision must be made in the cell. When BRCA1 and BRCA2 function properly, the cell can repair the damage through the normal HR pathway. If, however, either BRCA1 or BRCA2 are dysfunctional due to mutation, the damage is unable to be repaired by the error-prone NHEJ pathway that normally kicks in as a last resort. This inability to repair the DNA through NHEJ is due to the particular nature of these newly formed double-strand breaks. Dr. Ashworth and his colleagues found that when these breaks occur, cells trigger the self-destruct mode and die, rather than fix the broken DNA.
PARP Inhibition as a Cancer Treatment
Upon Dr. Ashworth and his colleagues finding that cells lacking BRCA1 or BRCA2 function were uniquely sensitive to loss of PARP function while normal cells were not, they began to probe whether this phenomenon could be utilized to treat BRCA-mutated cancers. Based on this hypothesis, they were then able to prove that treating cells lacking BRCA1 or BRCA2 function with pre-existing PARP-inhibitory drugs was able to prevent growth of these cells, similar to what they saw with cells without any PARP protein. They were also able to show that PARP inhibitors prevented the growth of BRCA2-deficient tumors in mice.
Dr. Ashworth’s laboratory determined that BRCA1- or BRCA2- deficient cells treated with PARP inhibitors were 50 to 100 times more sensitive to the PARP inhibitors than cells with functional BRCA1 or BRCA2 genes. These ground-breaking discoveries opened up an entirely new world of research that led to the eventual approval of three PARP inhibitors (PARPi) for the treatment of certain BRCA-mutated cancers, with more currently being tested in clinical trials.
The approval of PARPi for BRCA-mutated cancers is considered a massive advancement for cancer treatment. The recent FDA approval in January, 2018, of a PARP inhibitor called Olaparib for treatment of germline BRCA-mutated HER2-negative metastatic breast cancer, is the first targeted treatment for BRCA-mutated breast cancers. While the use of PARPi is currently limited to a few specific cancers, it has the potential to treat many more in the future.
The work for scientists, therefore, is not yet over. In addition to testing PARPi in other cancers, scientists are further probing the connection between PARPs and the HR repair pathway. Dr. Ashworth and other researchers believe that other proteins functioning in the HR repair pathway may share a similar relationship to PARP. Cancers that arise as result of mutations in genes that function in the HR pathway have similarities to BRCA-mutated cancers. Scientists are testing whether cancers with this quality, termed BRCAness, can also be treated with PARPi. The findings that many cancers have genetic deficiencies in common DNA repair mechanisms are beginning to show that cancers spanning many tissue types are more similar than previously thought.
The Future of PARPi Research
While the use of PARPi as a cancer treatment has been an exciting advancement, it has not been without its limitations. BRCA-mutated cancer cells have been shown to build up resistance to PARPi over time. Therapy-resistance is not unique to PARPi and occurs with many chemotherapies. Cells naturally develop resistance to drug therapies by accumulating additional mutations in their DNA. Resistance to PARPi, similarly, is often associated with reversion mutations in the BRCA1 or BRCA2 genes or in other genes in the HR pathway. Researchers are currently studying the mechanism of PARPi resistance in BRCA-mutated cells. My next article will delve into a recent study by Dr. David Quigley, a recipient of the BRCA Foundation’s Young Investigator Award, who works with Dr. Ashworth. Dr. Quigley’s research examined how resistance to PARPi arises in BRCA-mutated prostate cancer.
In summary, PARP proteins, like BRCA1 and BRCA2, are instrumental in repairing DNA damage. When both DNA repair pathways are impaired, cells cannot live because of the persisting DNA damage. PARPi uniquely effects cells unable to perform HR as a result of inactivation of the BRCA1 or BRCA2 function and does not harm healthy cells around it. The condition in which cells with a single genetic deficiency die when a second function is inhibited, but neither deficiency alone causes cell death, is called synthetic lethality. This unique condition results from impairing two redundant pathways that can normally compensate for each other. The discovery of synthetic lethality in BRCA-mutated cancers has sparked researchers to determine whether other sets of compensatory pathways are involved in cancer, giving hope for more targeted therapies.
The mechanism of PARPi in treating BRCA-mutated cancers has triggered the search for mutations that cause similar deficiencies in non-BRCA-mutated tumors. Early findings hint that BRCAness is far more widespread than previously imagined. Because DNA repair is so crucial to the wellbeing of our cells, it is not surprising that many cancers arise as a result of deficient DNA repair mechanisms. Targeting cancers with common deficiencies in DNA repair, whether they stem from mutations in BRCA1, BRCA2 or other proteins involved in HR repair, is proving to be a powerful way to specifically target a broad range of cancers. Understanding how cancer cells differ from non-cancer cells is giving us insight into the cause of cancer development. Further investigation of these underlying genetic differences will allow us to gain a new perspective of how many diseases are similar or different.
[1] Dr. Ashworth’s laboratory is currently funded, in part, by the BRCA Foundation
[2] As discussed in my previous post, BRCA: Bracing the Genome, the mode of DNA repair is dependent on the type of damage and the specific time in the cell cycle in which the damage occurs.